Before we discuss about the main topic for today, I'll be talking briefly about pregnancy dating.
Pregnancy is dated based on the last menstrual period, LMP (1st day of menstruation) and NOT the date of conception.
The mean period of gestation is around 280 days or 40 weeks, and hence the estimated date of delivery (EDD) can be calculated, by bringing forwards the LMP for 9 months and 7 days. This rule assumes that :
a) The cycle is of 28 days
b) It's a normal cycle (not conceived after stoppage of OCP/soon after previous pregnancy)
c) Ovulation occurs at 14th day of menstrual cycle
Hence, if the cycle is longer than 28 days, the number of days in excess must be added to the LMP.
In most antenatal clinics, gestational calender is available in assisting you in calculating the EDD. However, there's always a difference in a day or two compared to the previously calculated value.
Most mothers should have undergone their 1st ultrasound scan during the late 1st trimester or early 2nd trimester, for the purpose of :
a) Confirmation of pregnancy (intra/extra-uterine)
b) Pregnancy dating
c) Ensure that the pregnancy is on-going
d) To determine the chorionicity
Pregnancy dating done using USG method before 20 weeks of pregnancy is more accurate than any other methods used. However, after 20 weeks of pregnancy, dating done by USG is not reliable, since there's a variability in terms of the growth of different fetuses.
Here's an example of a History taking templete :
1) Patient's profile
Age
Occupation
Briefly described about the ethnicity background
Presenting problems
2) History of present pregnancy
Period of gestation, EDD and LMP
Results of dating done by USG
The chorionicity of pregnancy (singelton, multiple)
Details of the presenting problems :
a) What actions have been taken for tackling this problem
b) Are there any other plans for the rest of this pregnancy
c) What are the main concerns of the mother?
Is there other problems present?
Is there any h/o of PV leakage, bleeding? Any contractions felt?
3) Ultrasound
How many USG scans done?
Are there any problems?
4) Past Obstetric history
Past obstetric history provides the most important information regarding the risks of current pregnancy.
The details about past pregnancies is recorded, which includes :
Year, period of gestation, chorionicity, mode of delivery, outcome, any pueperial complications, and status of child currently.
Particularly important information includes :
a) H/O of recurrent miscarriages (risk of miscarriage and IUGR in current pregnancy increases)
b) H/O of abruption (risk of recurrence)
c) H/O of giving birth to a child with congenital anomalies
d) Unexplained still birth previously (may be related to gestational DM)
e) H/O of IUGR in previous pregnancies
f) H/O of macrosomia in previous pregnancies (gestational DM?)
g) H/O of pre-term delivery previously
h) H/O of early onset of pre-eclampsia (risk of pre-eclampsia and IUGR in this pregnancy increases)
Now, record the parity index.
Gravida = number of pregnancies regardless of the outcome
Parity = number of live births and still births after 24 weeks
In a twin pregnancy, it's counted as 2.
For example, a women with twin pregnancy, currently in 26th week of gestation. Parity index = G1P2
Another way of recording the parity is by noting down the parity index as usual, followed by the number of pregnancies not resulting in a live birth or still birth after 24 weeks.
5) Past gynaecological history
Prolonged menstrual cycles, may be related to Polycystic Ovarian Syndrome, which these womens are of high insulin resistance, increases their risk of having GDM
H/O of OCP intake, especially when conception occurs right after the stoppage of OCP intake. This renders difficulty in pregnancy dating.
Or sometimes, women may conceive when the Intrauterine devices are still in-situ, which increases the risk of ectopic pregnancy.
H/O of previous episodes of Pelvic inflammatory disease (PID) may result in ectopic pregnancy. Important to ask whether these genital tract infections have been treated adequately (and her partner)
When is the last pap smear done?
Yes, every year cervical cancer is detected in small amount of pregnant women.
If the pap smear is normal, have there in incidence of previous abnormalities?
What have been done for such abnormalities?
For eg, in Knife Cone Biopsy, it increases risk of cervical imcompetence and cervical stenosis (pre-term delivery and dystocia)
Any h/o of ectopic pregnancy? If yes, where is it? What have been done?
H/O of ectopic pregnancy increases the risk of recurrence in current pregnancy for 1 in 10.
Any h/o of multiple 1st trimester termination of pregnancy?
This increases the risk of pre-term delivery
Any h/o of surgery done in the uterus?
Any pelvic masses present? (fibroids/cysts)
Is the present conception assisted?
This increases the risk of multiple pregnancy and pre-term delivey
6) Past medical and surgical history
Major medical illnesses that have a major impact to the current pregnancy :
a) Diabetes mellitus - macrosomia, IUGR, Intrauterine death, congenital anomalies, neonatal hypoglycemia
b) Hypertension - pre-eclampsia, IUGR
c) Renal diseases - worsening of renal diseases, pre-eclampsia, IUGR
d) Epilepsy - frequency of fits increases during pregnancy
e) Venous thromboembolic disease - risk in pregnancy increases
f) HIV infection - vertical transmission
g) Connective tissue disorders - miscarriages, pre-term delivery, IUGR
h) Neuromuscular disorders (myasthenia gravis/dystrophia myotonica) - fetal neurological effects and muscle fatigue during labour
Previous surgical history - what anasthetics are used? Is there any complications?
Is there h/o of post-partum depression?
Is there h/o of non-pregnancy related depression?
Any other major psychiatric illness?
7) Family history
Diabetes mellitus, hypertension, thromboembolic diseases, psychotic disorders, genetic problems, congenital anomalies
8) Drug history
Any medications, including over-the-counter drugs and traditional medicine
9) Allergies
Any food/drug allergies, and what are the effects
General examination
1) Weight and height
Weight measurement is to detect any underweight and overweight mothers.
Any pregnant women with BMI <20, risk of IUGR and perinatal mortality increases, particularly if the weight gain during pregnancy is poor.
On the other hand, those with BMI >30 (obese), those are at risk of GDM and pre-eclampsia, and fetal assessment is more difficult (palpation and USG). On top of that, there's risk of excessive birth weight, perinatal mortality increases.
Measurement of height initially only aids in calculating the BMI.
However, later if there's IUGR/macrosomia, measurement of heights and plotting it into various curves aids in accurate diagnosis of IUGR/macrosomia.
2) Blood pressure/Vital signs
Measure the blood pressure either in semi-reccumbent position or sitting up position. Any BP > 140/90, detected first during pregnancy, on 2 occasions, at least 4 hrs apart, the cause of hypertension must be investigated (although in 90% of the case, it's essential hypertension)
Proceed to measuring other parameters of vital signs -> temperature, pulse rate, and respiratory rate.
3) Check for signs of anemia
4) Examine if there's any thyroid swelling
5) Auscultate the chest (CVS and RS)
6) Breast examination
7) Abdominal examination
First, position the patient is semi-reccumbent postion, since most of them in their late trimesters or those having multiple pregnancies won't be able to lie down flat/supline.
Cover their legs with sheet, and request a caperone.
Inspection :
Comment on the shape of uterus, and if there's any asymmetery.
Any visible fetal movements?
Any scars? If surgery performed long time ago, mothers might not mention it to you.
RIF scar - appendicectomy
Suprapubic scar - C-section, laprotomy to remove pelvic masses/ectopic pregnancy
RUQ scar - cholecystectomy
Striae gravidarum and linea nigra (faint brown line extending from the umbilicus to the pubic symphysis)
Palpation :
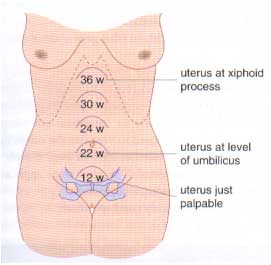
First, measure the symphysio-fundal height (SFH).
Gently palpate for the top of the uterine fundus, then feel for the upper border of pubic symphysis. Use the measuring tape, with centimetres down, measure the SFH and plot in under the symphysis-fundal height graph.
Many clinicians thought that SFH = period of gestation in weeks, but actually SFH in 2cm less then POG.
Large SFH = wrong dates? macrosomia? polyhydramnios? missed multiple pregnancy in USG?
Small SFH = wrong dates? IUGR? oligohydramnios?
Then, perform the fundal grip, lateral grip (limbs and spine), and pelvic grip.
Determine the number of fetal poles, which can be either the fetal head or bottom.
If there's only 1 or 2 poles, it's usually a singelton pregnancy.
If 3 or more poles are felt, it can be a multiple pregnancy or even a pelvic mass (fibroids/cysts) -> will be evident in history usually
Fetal lie is only determine when period of gestation is beyond 34 weeks, where it's defined as the relation in btw the fetal spine to maternal spine.
If fetal pole is felt over the pelvis, regardless of the position of the other pole, it's considered as longituidinal lie.
If fetal pole is not felt over the pelvis, just to one of the side, it's considered oblique.
If the fetal spine is perpendicular to the maternal spine -> transverse lie.
Now, again, if POG is > 34 weeks, you need to determine the fetal presentation.
It's usually cephalic (heads down) or breech (foot/bottom down), where the former is firmer than the latter.
If you've determine the presentation is cephalic, try determine whether it has engaged or not, by noting the number of fifths of the fetal head palpable.
If the entire fetal head is palpable, which renders it mobile, it's recorded as 5/5. It's considered engaged if only 2/5 or 1/5 of fetal head palpable, which is non-mobile.
Don't try to determine the fetal position, where it's only of important during onset of labour and only of significance when the progression of labour is slow.
If the fetal parts are too easily palpable + low SFH -> oligohydramnios
If the fetal parts are hard to feel + large SFH -> polyhydramnios
Auscultation :
If you're using a Pinard's fetoscope, place it over the fetal shoulder to listen to fetal heart beat. (normal 120-160)
Or it's better to use the hand-held doppler device since it can be appreciated by the mother.
Category:
Obstetrics Notes











POST COMMENT
0 comments:
Post a Comment