The Aims of antenatal care :
1) To detect, prevent, and manage the risk factors which adversely affects both mothers and fetus
2) To provide advice, reassurance, education and support to both mothers and family members
3) To deal with minor ailments encountered by mothers during pregnancy
4) To provide a general health screening
To determine the possible risk factors in the current pregnancy. the only way is by repeated history taking, examination and investigations. The first risk factor assessment is done during the booking visit, and of course, before the starting the assessment, the pregnancy must be confirmed and accurately dated. Any risk factors identified will be referred to a hospital-based or share-based care.
Booking visit
1) Confirmation of pregnancy
Symptoms of pregnancy (amenorrhoea, nausea and vomiting, breast tenderness and urinary frequency) together with a positive urinary/serum pregnancy test is usually sufficient to make a diagnosis.
However, most of the mothers are subjected to a "dating" ultrasound scan for confirmation of pregnancy and to accurately date it.
Fetal heart sound can be appreciated (either by fetoscope/hand-held doppler devices) by 12th week of pregnancy onwards.
2) Pregnancy dating
To determine a reliable EDD is important, especially in terms of pre-term gestation and prolonged pregnancy.
EDD can be determined by 2 ways :
a) From Last menstrual period (LMP)
EDD can be calculated from LMP based on the Nagele's rule.
This is done by addition of LMP with 9 months and 7 days, with few assumptions :
Accurate recollection of LMP
Menstrual cycle is normal and regular
Cycle length is 28 days
Ovulation occurs at the 14th day of menstrual cycle
However, there's tremendous drawback regarding the usage of Nagele's rule.
There's marked variability in terms of day of ovulation, cycle length, and the regularity of menstrual cycle.
b) Ultrasound scan "dating"
Hence, this is resolved by ultrasound "dating".
The benefits of such ultrasound "dating" :
i) To accurately determine EDDs of women with irregular menses, cycle length greater or lesser than 28 days, variability in terms of day of ovulation, inability to recollect LMP
ii) Maximises the potential of serum testing for fetal abnormalities
iii) To reduce incidence of labour induction for prolonged pregnancy
iv) For early detection of any multiple pregnancies
v) To determine if there's any asymptomatic failed intrauterine pregnancy
Such dating utilising USG scanning is most ideally done before 15th-16th week of pregnancy, since there's a negligible variation in terms of fetal size during this period. Hence, by determining the Crown-Rump Length (CRL), Biparietal diameter (BPD) and Femoral length (FL) using the USG scan, and plot it to the fetal biometry charts, the period of gestation and EDD can be accurately determined.
If the menstrual EDD differs from the scan EDD greater than 7 days, the scan EDD will be adopted as the final EDD.
However, after 20th week of pregnancy, dating using USG scanning becomes progressively inaccurate. Since starting from the 20th week, there's increased amount of fetal growth variability due to enviromental and genetic influence.
The booking history
All obstetrics, gynaecological, medical, and surgical should be eilicited in depth, as it may influence the outcome of the current pregnancy. Occasionally, the family and social history may have a greater impact towards the current pregnancy than the clinical factors.
Both extremes of ages, which is :
Age < 18 years -> increased risk of pre-term delivery and low birth weight babies
Age > 35 years -> increased risk of chromosomal abnormalities (Down Syndrome)
Certain racial/ethnic groups are of higher risk in developing certain genetic diseases (Sickle cell anemia/Thalassemia) and others (fibroids in African women).
Past medical history
The interaction in between pregnancy, medical, surgical and psychiatric conditions giving rise to a clinical specialty, known as Maternal medicine.
Important medical ailments during pregnancy includes :
Diabetes, Hypertension, Renal diseases, HIV infection, Connective tissue diseases, Neuromuscular diseases (Myasthenia gravis, Dystrophic Myotonica), Venous thromboembolic diseases, and Epilepsy
Past obstetric history
Any complications during previous pregnancies are likely to reccur.
Hence, any problems in previous pregnancies are likely to influence the management of the current pregnancy.
Details regarding previous labour and deliveries should be sought on, as it may determine the mode of delivery in current pregnancy.
Important histories includes :
Recurrent miscarriages
Previous abruption
Early onset of pre-eclampsia
Intra-uterine growth restriction
Macrosomia
Unexplained still birth
Previous pre-term deliveries
Previous congenital abnormalities
Past gynaecological history
If there's history of infertility or recurrent miscarriages, one must consider the amount of psychological impact to the mother and her perception regarding the current pregnancy.
Even, history of recurrent miscarriages may be a marker for IUGR, pre-eclampsia, or any chromosomal abnormalities.
History of myomectomy may cause uterine weakness, leading to increased risk of uterine rupture during labour process.
History of cone biopsy for cervical cancer, increases the risk of cervical incompetence and cervical stenosis (risk of preterm delivery and dystocia)
Important information includes :
Menstrual abnormalities
History of OCP intake/Usage of intrauterine devices
History of pelvic inflammatory diseases (PID)
Cervical cancer detection
Intervention done for abnormal cervix (Cone biopsy)
History of ectopic pregnancy
History of recurrent miscarriages
History of multiple 1st trimester termination of pregnancy
Uterine surgery done/Pelvic masses
Assisted conception (IVF, etc)
Family history
Risk of gestational diabetes for mothers increases if there's family history of type II diabetes mellitus.
As well as family history of hypertension, thromboembolic diseases.
Psychotic psychiatric disorders in family members increases risk of post-partum blues among mothers.
Genetic diseases that runs in family, and congenital anomalies in family members.
Social history
Smoking/Alcohol intake/Drug abuse
The marital status of mother
Current occupation (partner's as well)
Anyone in the family to look after the mother?
Is there any housing problems?
Distance of residence from the nearest hospital
The booking examination
First, as mentioned in previous post, Weight and height measurement.
To determine mother's BMI.
Blood pressure measurement, with other parameters of vital signs.
General and Abdominal examination (as in previous post)
The booking investigations
Urine
a) Asymptommatic bacteriuria
Asymptommatic bacteriuria may ascend up to the upper urinary tract causing acute pyelonephritis, which may impose significant morbidity of both mothers and fetus (increased risk of pre-term labour or even miscarriages)
Hence, all pregnant women during their booking visit, should have either their MSU being cultured or urinary dipstick done for nitrates (UTI).
b) Others
On top of that, dipstick test should include detection of blood, glucose and protein in urine.
Blood
a) Full blood count
2 most important parameters : Anemia and Thrombocytopenia
Anemia in pregnancy is usually caused by iron deficiency.
However, presence of thrombocytopenia, Hb < 9gm/dL or persistence of anemia despite intake of hematinics requires further investigations. (for eg : Hb-electrophoresis)
b) Blood grouping and Rhesus Status
Blood grouping is done during booking visit in case there's any emergency later, to aid in cross matching of blood. Presence of red cell antibodies is usually caused by previous blood transfusion, which may be problematic during rapid cross matching later, or even results in Hemolytic disorders of newborn (HDN) due to ABO incompatibility or Rhesus isoimmunisation.
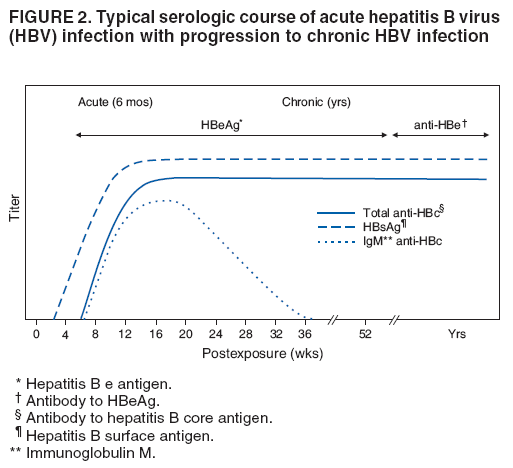
c) Hepatitis B serology
If HbsAb is positive, it means either the mother has previous Hep B infection, or she's immunised against Hep B, which is not of significance.
However, if HbsAg is positive, it means either there's a recent infection or the mother is a carrier.
Risk of vertical transmission is high, and even horizontal transmission is possible among medical staffs and newborn infants if there's a contact with these bodily fluids.
A newborn infant should be actively and passively immunised against Hep B after birth.
d) HIV serology
Less than half of the mothers are aware of their HIV status, until screening test is done.
Currently, all pregnant mothers are subjected for HIV screening during their booking visit.
If a mother is HIV positive, the risk of vertical transmission can be reduced from 30% to less than 5% by :
a) Avoid vaginal delivery (plan for C section)
b) Avoidance of breast feeding
c) Given HAART treatment
e) Syphilis (VDRL)
Incidence of syphilis is increasing recently, it's serious implication to both mothers and fetus, and due to the fact that syphilis can be adequately dealt in both mothers and fetus, simply be a course of antibiotics, VDRL screening is done for all pregnant mothers in this country.
f) Screening for gestational diabetes mellitus
In Malaysia, only mothers with risk factors for GDM will be screened.
Will be dealt in detail when GDM is discussed later.
Cervical smears
Pap smear will be done in pregnant mothers if :
a) Unlikely to attend postnatally
b) Due date for pap smear
c) Abnormal cervix during examination
Fetal abnormalities screening
This will be dealt in detail during discussion of pre-natal diagnosis.
Bear in mind that these screening test are optional, done only after verbal consent is obtained and the pros and cons of such screening test are explained to the mother.
Such screening test includes :
Nuchal translucency test (11th-13th week) and Serum testing (15th-19th week) for Down's Syndrome
Serum alpha-fetoprotein screening test for neural tube defects (eg : spina bifida, anacephaly) done during 15th-19th week
Detailed Ultrasound Anomaly scan (19th-22nd week) done to detect any congenital structural defects
Follow-up visits during antenatal period
The recommended frequency of antenatal visits are :
Upto 32nd week of pregnancy : every month
32nd-36th week of pregnancy : every fortnight
36th week till delivery : every week
However, according to the Royal College of Obstetrics, at least 5 antenatal visits are required in :
12th week
20th week
28th-32nd week
36th week
40th-41th week
During subsequent antenatal visits, the following must be done :
1) History taking to assess the maternal well-being
2) Enquiry about fetal movements (from 24th week)
3) Blood pressure measurement
4) Oedema assessment
Oedema is a common problem during pregnancy and is an insensitive indicator of pre-eclampsia.
However, if oedema occurs at abnormal sites, such as face, hands, vulva, etc, it might be sinister.
5) Urinalysis
For detection of blood, glucose, protein and nitrates. (UTI, pre-eclampsia, GDM)
6) Full blood count should be repeated during 28th and 34th week.
7) Abdominal examination - to record SFH
8) Auscultation of fetal heart sound (can be done using fetoscope or handheld doppler devices)
9) If the period of gestation is 36th week and above, fetal lie, presentation and the extent of engagement should be determined. This is the time when the mode of delivery is being determined.
10) If the period of gestation is 41th week and above, details about induction of labour should be explained to the mother. Labour induction is usually done 12 days after EDD.
Common problems detected during antenatal visits :
Gestational diabetes mellitus
Pregnancy-induced hypertension
Small for dates
Large for dates
Abnormal presentation
The cut-off point for pregnancy induced anemia is Hb level of < 10.6 gm/dL.
Usually, all pregnant mothers are given hematinics. The common complain about hematinics is usually regarding it's gastrointestinal intolerance, nausea/vomiting.
Iron syrups can be given instead of tablets if such problems occurs.
If oral therapy fails, IM injection of iron preparation may be necessary.
During antenatal visits, mothers should be express their concerns and anxieties to the consultants, and some maternal education should be done, regarding feeding and parenting skills, details of deliveries, problems during puerperial period, and etc.
Category:
Obstetrics Notes














POST COMMENT
0 comments:
Post a Comment