Briefly about anatomy of anal canal
The anal canal commences from the level where the rectum passes through the pelvic diaphragm towards the anal verge. The junction in between the anal canal and rectum is the anorectal ring/bundle which can be felt during PR examination.
The internal sphinchter is a circular, non-striated, involuntary muscles innervated by autonomic nerves.
The external sphincter is striated, voluntary muscles innervated by pudendal nerves.
The superior part of external sphincter fuses with the puborectalis muscle to form the anorectal bundle, for maintainance of continence.
The lower part of anal canal is lined by the sensitive squamous cell epithelium
The lymphatic drainage of the lower half of anal canal is drained into the inguinal lymph nodes
Blood supply - superior, middle and inferior rectal vessels.
Haemorrhoids
The anal canal contains 3 anal cushions, which serves as a gas-fluid protective barrier and closes it. When these cushions enlarge, they can prolapse, and when they're damaged, it causes bleeding.
Chronic hemorrhoids produces pile mass, as the processes are compressing on the perianal skin below it, produces external skin tags.
How it cause bleeding?
As these vascular pads becomes haemorrhoids, they assumed into a position closer to the anorectal junction.
During defecation, as the anal canal everts, the stools compressed against the vascular pads, scratching the mucosa over it.
After defecation, the vascular pads are remained scratched, and hence, blood start to trickle down.
If the vascular pads are unable to reduce after the anal sphincter closes, it worsens the bleeding by impairing it's venous return.
Symptoms (History)
Usually seen in individuals > 20 yrs of age. Extremely rare in children.
Bear in mind that uncomplicated piles are not painful.
Hence, it usually causing painless PR bleeding, which can be mild (notice on wiping your ASS after shitting), or can be severe to the extent of splashing all over the lavatory and eventually causing iron deficiency anemia.
Due to mucus discharge from the surface of hemorrhoids, it can cause pruritus ani.
Another important symptom is sensation of prolapse after defecation, or palpable lump. This forms the basis of the classification of piles based on the severity of prolapse :
Grade 1 : Only bleeding, no prolapse
Grade 2 : Prolapse occurs, but reduces spontaneously
Grade 3 : Doesn't reduce spontaneously (reduce manually)
Grade 4 : Irreducible
However, such classification is artificial, since every hemorrhoids prolapsed during defecation, the only way where it leads to bleeding.
Hence, to translate it clinically :
Grade 1
Prolapse occurs during defecation, but reduces back to it's normal position when the anal sphincter closes. Hence, no lump is noticed by the patient.
Grade 2
The prolapse occured during defecation, reduces back spontaneously but slowly.
Only complicated piles, when it strangulates, thrombosed, becomes gangrenous, fibrosed causing pain. Also known as acute hemorrhoidal crisis.
If the patient has any underlying coagulopathy, bleeding disorders, or taking aniticoagulants, piles may bleed massively.
Examination
Don't ever forget that non-prolapsed/thrombosed piles can't be diagnosed by your fingers! It's indistinguishable from normal mucosa.
Hence, a sigmoidoscopy/proctoscopy is very much required.
However, 3rd/4th degree hemorrhoids, since it's visible, you may be able to make a spot diagnosis.
It's a bluish-purplish swelling, with diameter of 1-2cm, with soft mucosal surface, usually non-tender (unless complicated), with mucus-exuding surface.
If it's complicated, it'll be tense, tender, oedematous.
Sigmoidoscopy and proctoscopy is still required to rule out other rectal pathology.
Management
For acute hemorrhoidal crisis, many surgeons thought that surgical intervention at this stage may cause portal pyemia.
But, it's not true -> if early antibiotic coverage is given.
Yet, many surgeons usually wait until the acute phase is over, and then only decide whether hemorrhoidectomy is required.
During acute phase :
Analgesics given.
Apply cold/warm saline bag pressure -> mass usually shrinks after 3-4 days
For 1st-2nd degree haemorrhoids :
Give defecatory advice - only shit when the desire is there (don't simply shit), apply correct shitting position to minimise straining, in addition of stool softerners and bulk forming agents.
Not responsive -> Submucosal injection of 5% phenol in almond oil
Indications of hemorrhoidectomy
1) 3rd-4th degree
2) 2nd degree non-responsive to non-operative management
3) Fibrosed haemorrhoids
Perianal hematoma
It's actually a misnomer, since it's not a true hematoma.
It's caused by thrombosis of a subcutaneous veins within the anal tissue, secondary to injury of venous wall while straining on defecation.
The thrombosis subsequently causing inflammation and edema of the surrounding tissues.
History
Age
Any age, no sexual predilection
Symptoms
Characterised by anal pain, which gradually increases in it's intensity over hours, and subsides after a few days. It causes a continuous discomfort, worsened by sitting, walking, etc.
It is associated with the presence of a lump in the anus, which initially small in size, and gradually enlarges when it becomes more painful.
If the lump ruptures through the skin, or it ulcerates, it can cause PR bleeding.
Since it causes partial opening of the anus, as there's continuous mucus discharge, it results in pruritus ani.
Can be triggered by episodes of straining at stools while defecating.
Signs
The lump can be located anywhere along the anal margin.
The skin over it appears reddish-purplish.
Size is usually small initially (1x1cm), with hemispherical shape, gradually enlarges in size, which becomes polypoidal.
With smooth surface, hard in consistency.
It's tender, but disproportionate to what the patient complaints of.
Not fix to the skin, nor it can be reduced back into the anal canal.
Local/regional lymph nodes are not enlarged.
Fistula in ano
A fistula is a track, lined by squamous epithelium/granulation tissues, connecting two epithelised surface, either in between 2 body cavities, or 1 body cavity - external skin surface.
Hence, fistula in ano is an abnormal, fistulous connection between the rectum or anal canal to the external skin. Usually caused by a ruptured intersphincteric abscess. It has an external opening on the skin, and an internal opening, which can be classified based on it's relative position to the anorectal ring :
High level fistula
Internal opening located above the anorectal ring. As it tracks through the anorectal bundle, it causes incontinence. Different varieties of it includes :
Extra-sphincteric, Trans-sphincteric, Inter-sphincteric
Low level fistula
Internal opening located below anorectal ring. It doesn't cause incontinence.
Different varieties includes :
Trans-sphincteric, Inter-sphincteric, Subcutaneous/Submucosal
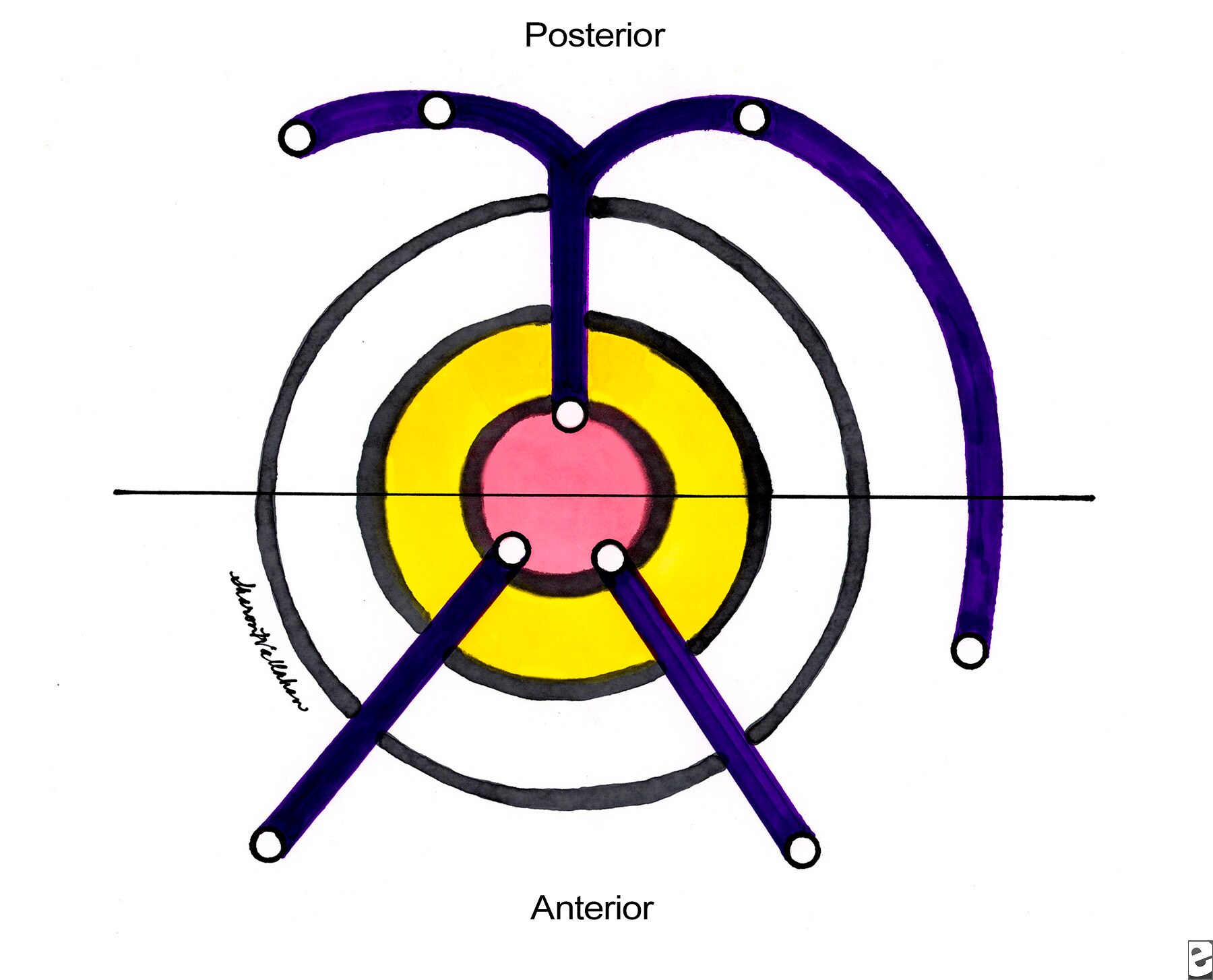
Goodsall's rule
According to goodsall's rule, any anterior fistula will have it's internal opening located along a line drawn radially, connecting the external opening to the anus.
Whilst any posterior fistula, regardless of it's position, will have is internal opening, located at the posteior anus, on midline position.
History
Patient may have h/o of perianal abscess, might have been drained or healed.
Commonest symptoms is watery, serous, purulent discharge from the external opening.
They may complaint of bubbling sensation during defecation, as stool passes through the anal canal, it forces mucous discharge from the fistula. This also prevents healing of the fistula.
Periodic throbbing pain can be there as pus accumulates within the tract.
Persistent mucous discharge causing pruritus ani.
Some amount of bleeding might be there. (from external opening)
In your history taking, also ask for symptoms of inflammatory bowel disease, any abdominal upset, systemic upset.
On examination
You'll notice that the discharge can be either serous or pustulous.
The external opening is seen as tufts of granulation tissues or puckered scars.
Rectal examination is usually not painful.
The internal opening is felt as an area of induration or a nodule under the anal mucosa. Most of the time, the tract is palpable.
Look for any other evidence of Anal carcinoma, TB, or IBD.
Confirm your examination findings using sigmoidoscopy/proctoscopy.
If the inguinal nodes are enlarged -> either due to infection of the fistulous tract, or infiltrative anal carcinoma.
Treatment : Fistulotomy, Fistulectomy
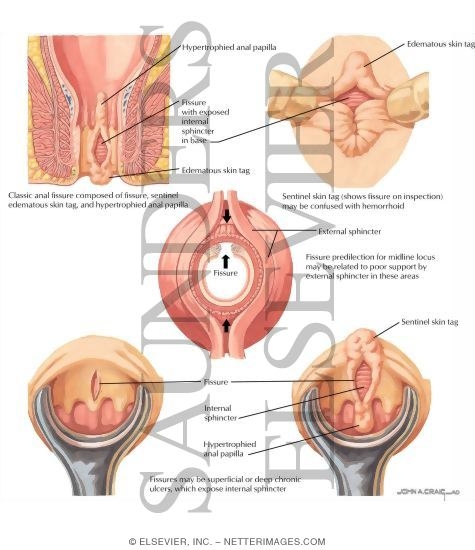
Anal fissure
Defined as a longituidinal split in the anal skin.

Acute tear is common, especially when there's excessive straining during defecation (hard stools?), and it usually heals rapidly. But during next defecation, as the stool stretches the anal canal, it causes the split to gape, leading to pain and bleeding. Then, it's so painful that the anal sphincter undergoes spasm.
Hence, a viscious cycle of tear-pain-spasm occurs, and produces further pain. Eventually, as the fissure becomes chronic, fibrosis occurs and a chronic ulcer is produced.
History
This condition can be quite common in children as they frequently passes bulky stools rapidly.
In adults, usually occurs in between 20-40 yrs of age, slightly more common in males. In females, might be seen after delivery.
Severe anal pain on defecation is the chief complaint, which is tearing in character. Persistent, throbbing pain is there minutes or even hours after defecation. It's sometimes so painful that the patient might be apprehensive towards defecation, and ended up accumulating large volume of hard stools within the rectum. This only causes more pain during next defecation.
Since there's spasm of anal sphincter, patient might find it difficult to pass motion. (As for laymen, constipation)
There's streaking of stools with blood, or the patient notices blood while wiping their ass after defecation. As with chronic fissure, there's only mild-bleeding.
In chronic fissures, sometimes there's a sentinel-skin tag palpable at the lower end of the fissure. And due to the hypertrophy of the anal papillae, mucus discharge from the ulcer causing pruritus ani.
Examination
Most anal fissures are located at the posterior midline of anal skin, some at the anterior midline, rarely lateral.
Usually diagnosed by separating the anal skin, and the split is visible.
Rectal examination is usually not possible as it's too painful.
However, if it's not too painful for the patient, anal skin defect can be felt during examination, surrounded by area of induration.
NO proctoscopy/sigmoidoscopy should be done on a conscious patient !!!
Category:
Surgery Notes
















POST COMMENT
0 comments:
Post a Comment